A Family Doctor's Voice Into the Madness
 As a primary care physician, I feel like I need to speak
some scientific truth into the madness that I am reading lately on the internet
about Covid 19. My hope is to provide
reason which is not delivered in super science language, but with accuracy and
accessibility. Please feel free to do whatever you would like with this
information.
As a primary care physician, I feel like I need to speak
some scientific truth into the madness that I am reading lately on the internet
about Covid 19. My hope is to provide
reason which is not delivered in super science language, but with accuracy and
accessibility. Please feel free to do whatever you would like with this
information.
Covid 19 is the illness complex caused by SARS-CoV-2 the
newest bad boy coronavirus on the block, in the same family as SARS and MERS as
well as the common cold types of coronavirus.
ILI = Influenza like illness
Regarding testing:
Currently we have several forms of testing available and
hopefully new testing forms will be developed soon. The PCR test that is mentioned has both a
slower turnaround form and a few that are rapid. PCR tests are obtained by swabbing the nose,
or the very back of the nose/upper throat, and one form is done through
spit. The samples are collected and
placed in one of two different solutions and then run on machines that can look
for the RNA (genetic code material) in the middle of the Covid virus. These tests do have false negatives (meaning
that a person can be infected and the test is negative). These are not ideal to be used in clinics as
a widespread quick test, but are the best we have, and have to be run at
specific labs on very specialized machines which are tightly maintained. These tests are NOT ideal for wide spread
screening, but are the best we have currently at determining if a person has a
current infection. In Montana we
can now test anyone with symptoms of Covid, and asymptomatic people who are
going to have elective surgeries. Prior
to this week we have only been screening those deemed high risk, and healthcare
workers.

The antibody tests are under development now and some are
available commercially. They are looking
for evidence that a person has had the infection at some point in
the past. Most people don’t
develop measurable antibodies (their own proteins made by the immune system to
attack a virus) until at least 7 days into the infection. These are from blood tests, and currently
there are only a few approved by the FDA, though many are being offered by commercial
companies. If you have had a regular old
run of the mill coronavirus infection (which causes the common cold) you can
have an antibody test come up as positive without ever having had Covid 19. The false positives make these tests
difficult to interpret, and they also have the problem of false negatives as
well. Large centers are able to measure
antibody levels in those who have recovered from confirmed Covid, and those
people may be able to donate plasma for the treatment of currently sick
patients. Plasma treatment can only be
done between two people who share compatible blood types.
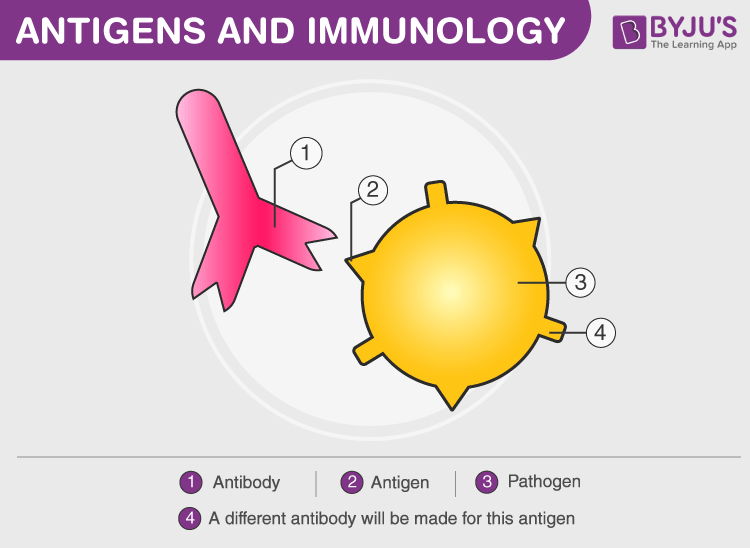
The newest tests being developed would be tests for antigen
of the virus. Proteins on the outside of
the virus that our bodies respond to and attack when fighting infections. Antigen tests are also done through swabs of the
throat, or nose, and would be able to be used in clinics without high tech
labs. They would allow us to determine
if a person has a current infection. They
are more like the tests we currently have for strep or influenza. These would allow much wider spread
screening, and will be necessary as time goes on in order for us to more fully
understand the extent of this virus.
Currently we start with antigen tests to screen a person for influenza
and if needed move onto the PCR tests for other viruses, including the flu,
when a person is hospitalized. Prior to
Covid, the back-up tests used after antigen tests for influenza cost about
$1800 and are not covered by insurance if a person is not admitted to the
hospital. More on this in just a moment.
Regarding Influenza-Like Illnesses:
There are four strains of influenza which typically
circulate every “flu season”. These can
be tested for with antigen tests at a walk in or doctor’s office. However the tests are only about 50%
sensitive, and so we know that a large number of people who walk in with an
influenza like illness (fever, cough, fatigue, sore throat, body aches,
headache) and have a negative test,
actually do have the influenza virus. Then
there are the other viruses that circulate during the same season, and cause
similar illnesses. Those are adenovirus, parainfluenza virus, human
metapneumovirus, and RSV. Each of these,
in addition to influenza, can cause lower respiratory tract (think lungs not
runny nose and sneezing) infections.
These will not show up on the routine office flu test, and can cause
remarkable illnesses. And then to
broaden the number of infections that come along with cold and flu season, are
all the cold viruses. These include, and
are not limited to, rhinovirus, enterovirus, coronviruses, etc. They don’t typically cause deeper lung
infections, but can cause more problems in people with lung diseases like
asthma, elderly people and in younger children.
Let’s say Sally, an otherwise healthy 45 year old female,
comes to see me in December with fever, cough, sore throat and body aches. She has pretty normal oxygen levels, but is
breathing a little faster than usual (which isn’t surprising given her
fever). I order a flu swab, and 10
minutes later it comes back negative.
Since she doesn’t have asthma, and prefers to avoid taking medications,
I send her home with rest, Tylenol alternating with Motrin, cough syrup, and
increased fluids. I also instruct her to
return if she develops difficulty breathing or coughing that limits her ability
to breath. Sally goes home on Friday from
my office, and by early Saturday morning she is having a really hard time
getting her breath, and feels like she can’t breathe. She will present to the ER and undergo blood
work, chest x-ray, and a viral respiratory panel (the expensive one). She
may get a breathing treatment and sent home, or she may be admitted, but most
likely she won’t need to be intubated and ventilated (tube in her throat and a
machine to breathe for her). It is very
likely that her respiratory panel will have influenza, or one of the other
viruses listed above…and sometimes patients even have 2 viral infections at
once which is why they do worse (after all in cold and flu season, there are
quite a few different viruses that circulate) .
She will likely spend a few days in the hospital, on the medical floor with
a little oxygen and some breathing treatments before discharging home and
resuming normal life.
Now Roger is a 35 year old man with moderately severe asthma, and he smokes. He comes in to see me in January with the same story. But on his exam he is wheezing and his oxygen levels are not as good as they should be. He's been sick for 2 days, and the people he works with were sick last week with a similar illness. I may not even bother with checking his rapid flu, because after an x-ray confirms he doesn't have an obvious pneumonia, I am going to send him home on flu meds, steroids, inhalers, and will be seeing him in my office in 2 days. He will also be instructed to present to the hospital if he worsens, but given that it is flu season, he's been around other sick people, and he is high risk, he gets treated, and close follow up. He may end up in the hospital even on flu medications and treatment for the flare of his asthma. But I make decisions on his care based on what I KNOW about influenza and the other ILI's and respiratory viruses. They are well understood, and 9 times out of 10 will behave in a certain pattern. Some of the ILI's, including influenza, can cause a non asthmatic to wheeze and require asthma medications. I have even seen some adults, with previously healthy lungs end up on inhaled steroids (like my 13 year old son with asthma) for up to 2 years! One seasonal, well known, irritating influenza-like virus can do that. While most people recover, some people like Roger and Sally up above can become very, very sick.
Now Roger is a 35 year old man with moderately severe asthma, and he smokes. He comes in to see me in January with the same story. But on his exam he is wheezing and his oxygen levels are not as good as they should be. He's been sick for 2 days, and the people he works with were sick last week with a similar illness. I may not even bother with checking his rapid flu, because after an x-ray confirms he doesn't have an obvious pneumonia, I am going to send him home on flu meds, steroids, inhalers, and will be seeing him in my office in 2 days. He will also be instructed to present to the hospital if he worsens, but given that it is flu season, he's been around other sick people, and he is high risk, he gets treated, and close follow up. He may end up in the hospital even on flu medications and treatment for the flare of his asthma. But I make decisions on his care based on what I KNOW about influenza and the other ILI's and respiratory viruses. They are well understood, and 9 times out of 10 will behave in a certain pattern. Some of the ILI's, including influenza, can cause a non asthmatic to wheeze and require asthma medications. I have even seen some adults, with previously healthy lungs end up on inhaled steroids (like my 13 year old son with asthma) for up to 2 years! One seasonal, well known, irritating influenza-like virus can do that. While most people recover, some people like Roger and Sally up above can become very, very sick.

These types of presentation of ILI's are common in the winter months.
And our hospitals manage without doctors and nurses themselves ending up on ventilators and needing high levels care.
We take care of patients, we get our flu vaccines, and if we get sick we
take meds, or just let them run their course.
Some years the flu seasons are particularly bad and hospitals will surge
above their capacity to some extent. In
Billings that can mean that we have about 35-60 more patients than usual. But still, the healthcare system stays
running and in pretty good order.
But I was sick this winter, it was awful, and I had a negative flu test….I
must have had Covid.
This is actually quite unlikely, unless you had been sick
this winter, say in December, in China.
But if you were in Montana or Kansas or middle America, not traveling extensively, or exposed to
those who had been in Wuhan in December, you were much, much, much more likely
to have had either a false negative in office flu test, or one (or two) of the many
other common viruses that occur from October through March every year. Your doctor didn’t likely offer you an $1800
test that your insurance wouldn’t cover.
They offered you reassurance, and you got better.
But there were so many people sick this winter, and they didn’t have
flu, so surely that was the early Covid peak.
Again, outside of some early traveling individuals, the
illnesses seen this winter were consistent with every other cold and flu season
we have had prior to Covid. People are
not keen to pay for high dollar viral
respiratory panels just to know for sure which virus they are sick with. As there is only one virus on that panel,
influenza, that has medications specifically to treat it. Most people, outside of high risk patients, like those with immune compromise and lung disease, recover from influenza, as well
as most other viral infections without anything more than TLC. That being said, when I have a patient with
suspected flu, risk factors, and a negative test I will often presumptively
treat with Tamiflu just to reduce their risk of moving on to more severe
illness and hospitalization. Do some of
them have another virus that won’t respond to that medication? Yes.
But the likelihood of benefit and lessening the risk of deterioration is
worth the potential side effects of the medication.
If we had an early “peak” of Covid this winter, our ICU beds
would have fallen short this winter. If
there had been an early peak your neighborhood healthcare workers would have been
dropping like flies, as sick patients spread the virus in high concentration,
and they also visit their doctors and nurses. I have never experienced a routine or even really horrible flu season in which doctors get online and solicit plasma from recovered flu patients to help treat their critically ill spouses, who happen to also be doctors, and cannot wean off of ventilators. Even in the most severe influenza seasons, healthcare professionals are able to continue to work as they also are likely to recover from the routine ILI's, or not get them because they get their flu vaccines, and already wash their hands to the point of cracking.
Covid is NOT just like any other influenza like illness. Yes, it causes deep coughing, fever, fatigue and body aches. It can also cause severe gastrointestinal illness (think 20 pounds weight loss in 10 days due to vomiting and diarrhea), renal failure, blood clotting issues, sudden cardiac death in otherwise healthy people, among other non common influenza-like findings. We did not have a peak of blood clotting, cardiac arrest, respiratory illnesses in our hospitals this winter. We did not have nursing homes admitting huge numbers of patients to the morgues this winter. There was NOT a Covid peak this winter. This virus cannot hide the destruction is causes.
Covid is NOT just like any other influenza like illness. Yes, it causes deep coughing, fever, fatigue and body aches. It can also cause severe gastrointestinal illness (think 20 pounds weight loss in 10 days due to vomiting and diarrhea), renal failure, blood clotting issues, sudden cardiac death in otherwise healthy people, among other non common influenza-like findings. We did not have a peak of blood clotting, cardiac arrest, respiratory illnesses in our hospitals this winter. We did not have nursing homes admitting huge numbers of patients to the morgues this winter. There was NOT a Covid peak this winter. This virus cannot hide the destruction is causes.
But it seems like there are really a lot more asymptomatic carriers
that don’t really get sick. The rate of
death is lower than we thought initially.
Thank God, the percentage of people with this virus who are
going to die is lower than we initially thought. However, numbers can be falsely
reassuring. The number of those people
with identifiable,
confirmed symptomatic infections (not asymptomatic carriers) who die, is still very
high. Meaning that those who actually
get sick are still at a good risk of profound complications as well as
death. Black and Hispanic people who get
sick are 3 times as likely to die as those of European decent based on what we
are seeing in NYC. And we don’t know why
that is. Men who get sick are more likely to die than are women. We don’t know why that is either.
The asymptomatic carriers are actually more frightening to
me than comforting. At least with all
the other ILI’s and cold viruses, we don’t see large numbers of people walking
around spreading the viruses without symptoms.
They are pretty easy to identify.
This virus hides in many, without causing symptoms, and they spread it
to those who develop illness with extreme efficacy. I would rather face an enemy I can see and
predict its behavior.
Influenza kills more people than this virus has…let’s just get on with
life.
Over the course of a year, influenza kills about 50,000
Americans. And that is with life as we
know it. We travel, work, go to school, vacation
and live life without restrictions for the most part during a normal flu
season. Life isn’t on hold. This virus has killed 46,497 Americans… in just
under 2 months, with the whole world on hold.
No dining out, no kids in school.
No churches meeting in mass. No
daycares. By the end of the week it will
be 7 weeks since the nation went on lockdown, an unprecedented lockdown. And by the end of this week 50,000 Americans
will have died. This is not
influenza. This is not just another one
of our routine influenza like illnesses.
It is different. SARS-CoV-2 is a
beast, and it is going to change the world as we have known it…for a while.
I will not be gathering to commiserate with people that
distancing is hard, I know it is. And
just because something is hard doesn’t mean that it isn’t worth it. I will not be the soft landing for pseudoscience,
nor will I be baited into debate over whether or not this virus is worth the inconvenience. For
the time being I will be leaving the safety of my home to continue to take care
of patients. I will be wearing a mask to
protect others from the chance that I may be a silent carrier of this
virus. I will not be shaking hands. I will be praying for the safety of my family
and friends. If you have questions
about ways to protect yourself or your loved ones I will be happy to help.


Comments
Post a Comment